Statistically, women report fewer orgasms than men. A study in orgasm frequency of US adults showed heterosexual men usually orgasmed during intimacy (95%) followed by gay men (89%), bisexual men (88%), lesbian women (86%), bisexual women (66%) and heterosexual women (65%). Women who orgasmed more frequently were more likely to receive more oral sex, have longer duration of sex, be more satisfied with their relationship, ask for what they want in bed, act out fantasies and express love during sex. Women were more likely to orgasm if their last sexual encounter included deep kissing, manual genital stimulation and oral sex in addition to vaginal intercourse.
Why the Orgasm Gap Exists
There are theories as to why women don’t orgasm as much as they’d like to. There is too much emphasis on penetrative sex. Our Western culture is goal oriented. For men the goal is to orgasm, and then the fun stops. Biologically, it’s more difficult for women to achieve orgasm from penetrative sex alone. According to sex experts 80% of women do not orgasm through intercourse alone. Most need direct clitoral stimulation to experience orgasm.
Female Orgasm During Intercourse
Fortunately there are ways to ensure women experience mind-blowing orgasms during sex. Penis in vagina intercourse is just one type of sex. Using your hands and mouth to arouse one another should be a central part of your sex life. Start with lots of full body touch. We recommend female orgasm or high arousal before penetration. Using your fingers in the vagina before inserting a penis can help warm her up. Emphasize clitoral stimulation before and during intercourse. The clitoris is the anatomical match to the penis, so just imagine men trying to reach orgasm without touching their penis and you’ll get a sense of how essential clitoral stimulation is to female orgasm. It can be easiest for her to keep touching her clitoris once intercourse has started.
The first moment of penetration can be exquisite and set the tone for the entire time. Make sure to not penetrate until she is ready. Try holding still and letting her slide onto the penis at her own pace, or going in one inch at a time. Wetness is not a good indicator of arousal. Women can be aroused but not wet, or wet but not aroused. Whenever it is needed, use good quality lube. Explore different depths, rhythms and speeds. Ask her what works well for her. Experiment with sensible sex positions. Focus on comfort and the ability to thrust and move easily. Take turns being the more active one. Try making sex last longer with foreplay, more attention to her pleasure, and gaining control over ejaculation. Have fun with extras such as holding still while she squeezes and releases pelvic muscles, make and hold eye contact, using full body touch during intercourse to maximize skin to skin contact. Adjust your erotic attitude from sexual scarcity to sexual abundance.
Four Ways to Close the Orgasm Gap
Explore the many, different kinds of female orgasm.


The Clitoral orgasm is from the clitoris, a small organ filled with nerve fibers that is derived from the same tissue in utero as the penis. It becomes erect and engorged with blood during sexual arousal. There are 2 sex positions that allow for more direct stimulation of it, the CAT (coital alignment technique) and the Reverse Cowgirl.
The Reverse Cowgirl sex position is one of the more well-known positions out there. Your man first needs to start by lying down on his back. You then get onto your knees, with one on either side of him, and lower yourself down on him while facing toward his feet. You lean against his upper thighs and grind against him to stimulate your clitoris. The CAT position is great if you like clitoral stimulation. You lie on your back with your legs open while your man is on top of you. But instead of thrusting in and out, you man moves forward so that the angle of the penis is more pointing downward so that his pubic bone will come into contact with your clitoris. It can also be performed with a strap-on.
The G-spot orgasm is from a sensitive area in the front wall of the vagina. When stimulated correctly, many women report intense orgasms that are different from clitoral orgasms. To stimulate the G-Spot curl two fingers into the vagina and press them into the upper wall in a come hither motion. Or slide 3 fingers into the vagina and sweep them back and forth like windshield wipers against the upper wall. The more you take the time to get to know your G-spot and what type of stimulation feels good, the more pleasure you’ll be able to derive from this erogenous zone.
The Blended orgasm is a combination of two or more different types, such as from stimulation of clitoris and nipple.
Anal orgasm involves intense pleasure from stimulation of nerves in the vagina and rectum. So for vagina owners, it may be possible for sexual arousal to occur from rectal stimulation. This definitely needs extra lubrication!
The Nipple orgasm can occur from breast stimulation as the nipple is an erogenous zone for many people and can lead to incredible orgasms. For men and women, nipple play is rewarding foreplay. A study showed that nipple stimulation enhanced sexual arousal in 82% of women and 52% of men. Nipples attract women, just like they do men. A University of Nebraska study found that women and men follow similar eye patterns when looking at women. They quickly look at breasts before moving on to other areas of the body. Piercing? In a study from 2008 94% of men and 87% of women polled about their nipple piercings said they’d do it again. They liked the look of it.
The Fantasy orgasm is possible if your brain is powerful enough to take your daydreams into orgasm territory with nothing more than naughty thoughts!
If you’re a fitness junkie, a Coregasm might be for you. Also known as exercise-induced orgasms, they occur during workouts, and may be due to vibrations from the abdominal and pelvic muscles.
Masturbate More


It doesn’t take two to have an exciting empowering sex life. Masturbation is good for your health and for improving your sexual encounters with your partner. There are numerous health benefits such as a boost of endorphins, reduced anxiety, a better sex life and increased blood flow to the vagina, which can reduce dryness and be especially helpful as you become older. Friction can cause discomfort, so using a lubricant (see pictures of two good brands) can help. For clitoral, try lying on your back. With a pillow under your head, spread your legs and start to rub your clitoris with whatever feels good. For vaginal, try squatting. Squatting makes it easier to find your G-spot, whjch is about 2-3 inches inside your vaginal canal. Slide your fingers or toy inside your vagina, moving deeper as you go. For anal, try face-down doggy style. The position gives you room to insert your fingers or toy in your behind with one hand while rubbing yourself with the other. For the combo, try the pretend lover. Think of the pretend lover as the cowgirl for one. Put your favorite dildo or vibrator on your bed, and lower yourself down until you find a sensation you like- either penetration, clitoral or both. Ride your toy as fast or slow as you want. At the same time rub your clitoris or play with your nipples. If you want to get your other senses involved, erotic stories can let you discover your sensual and sexual side. Check out literotica.com for some femme-friendly stories. If you’re more visual, watching porn can increase your libido and relieve stress in a safe way. If you like listening, audiobooks.com has steamy audio books. Masturbation is a fun, sexy and safe way to explore your desires and learn what turns you on.
Sex Toys Can Help Erase the Orgasm Gap

Some people think sex toys are for solo sex only, but using toys in the bedroom can be a shared experience, and can help take some pressure off when it comes to helping your partner orgasm. Toys come in all shapes and sizes, and many of them emit a range of vibrations that you can adjust to your need and desire. Three companies who sell sex toys are We-Vibe, Lelo and Tantus.
Communicate with Your Partner

To better communicate, demand you get what you need. Women are less likely than men to verbalize their sexual desires or speak up when they are not satisfied during sex. As for men, they assume that women all want the same thing in bed. All women are different with different wiring, different anatomy and different responses. If you feel awkward stating your desires during sex, you can start beforehand. Not sure what to say? Here’s a list:
The orgasm gap does not have to exist. Women deserve just as much pleasure as men. With a little attention to detail and more focus on female pleasure, you can narrow the gap for good, and that’s something worth getting excited about!







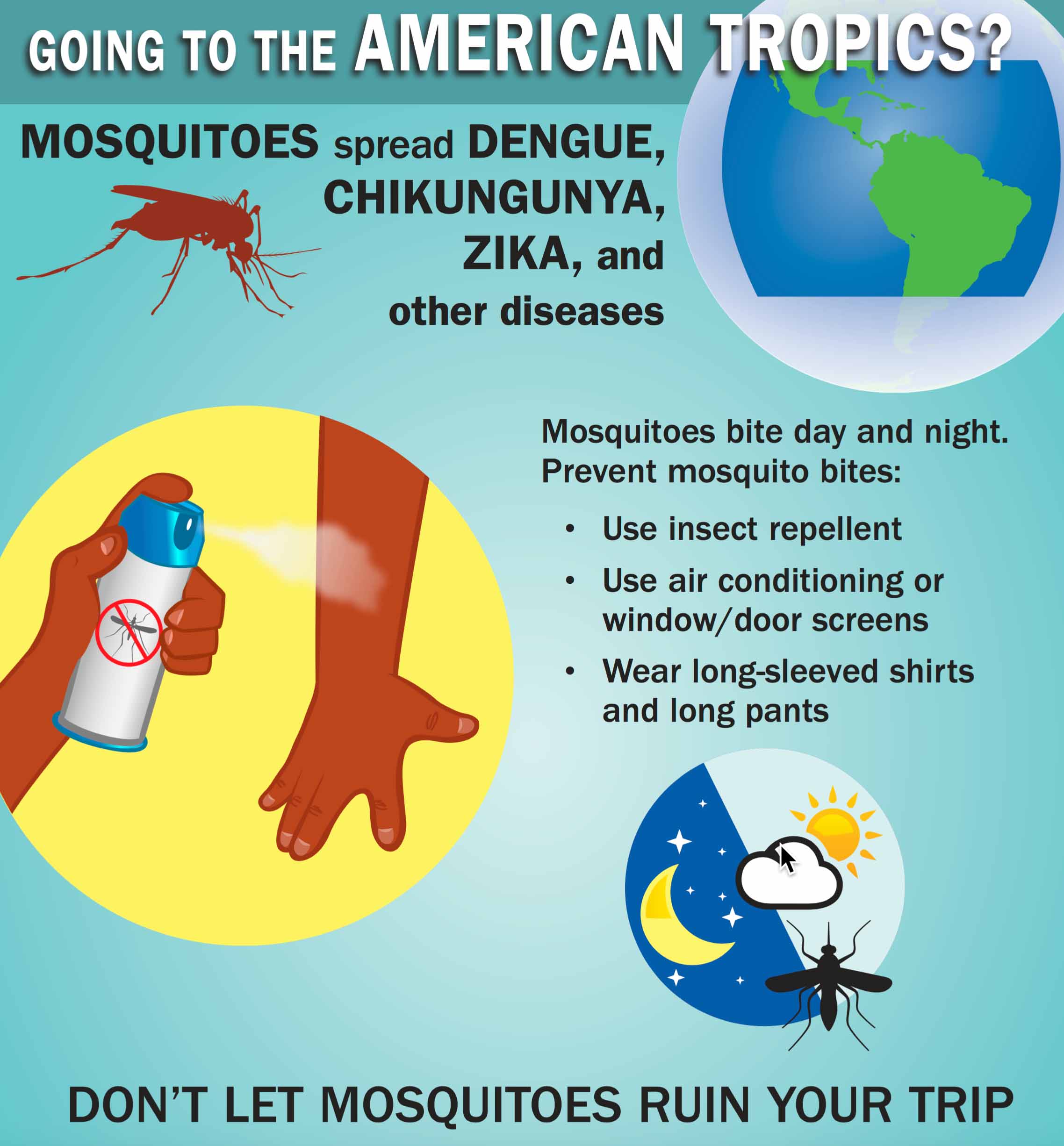
 Once a person is infected, the incubation period for the virus is approximately 3-12 days. Symptoms of the disease are non-specific but may include fever, rash, aching in joints, and eye inflammation. It appears that only about 1 in 5 infected people will have these symptoms and most will have mild symptoms. It is not known if pregnant women are at greater risk of infection than non-pregnant.
Once a person is infected, the incubation period for the virus is approximately 3-12 days. Symptoms of the disease are non-specific but may include fever, rash, aching in joints, and eye inflammation. It appears that only about 1 in 5 infected people will have these symptoms and most will have mild symptoms. It is not known if pregnant women are at greater risk of infection than non-pregnant. has been associated with birth defects, specifically significant microcephaly (small fetal head). Transmission of Zika to the fetus has been documented in all trimesters; Zika virus RNA has been detected in fetal tissue from early miscarriages, amniotic fluid, babies and the placenta. However, much is not yet known about Zika virus in pregnancy. Uncertainties include the incidence of Zika virus infection among pregnant women in areas of Zika virus transmission, the rate of transmission to the fetus, and the rate with which infected fetuses have complications such as microcephaly or demise. The absence of this important information makes management in the setting of potential Zika virus exposure (i.e. travel to active areas) or maternal infection, difficult. Currently, there is no vaccine or treatment for this infection.
has been associated with birth defects, specifically significant microcephaly (small fetal head). Transmission of Zika to the fetus has been documented in all trimesters; Zika virus RNA has been detected in fetal tissue from early miscarriages, amniotic fluid, babies and the placenta. However, much is not yet known about Zika virus in pregnancy. Uncertainties include the incidence of Zika virus infection among pregnant women in areas of Zika virus transmission, the rate of transmission to the fetus, and the rate with which infected fetuses have complications such as microcephaly or demise. The absence of this important information makes management in the setting of potential Zika virus exposure (i.e. travel to active areas) or maternal infection, difficult. Currently, there is no vaccine or treatment for this infection.